Bed Occupancy Calculator
Healthcare operations tool • 2026 edition
Bed Occupancy Formula:
Show the calculator\( BO = \frac{OC}{TC} \times 100 \times (1 + DF) \times (1 - EF) \times (1 + AF) \)
Where:
- \( BO \) = Bed Occupancy Rate (%)
- \( OC \) = Occupied Beds Count
- \( TC \) = Total Bed Capacity
- \( DF \) = Discharge Factor (turnover rate)
- \( EF \) = Efficiency Factor (utilization optimization)
- \( AF \) = Admission Factor (admission rate)
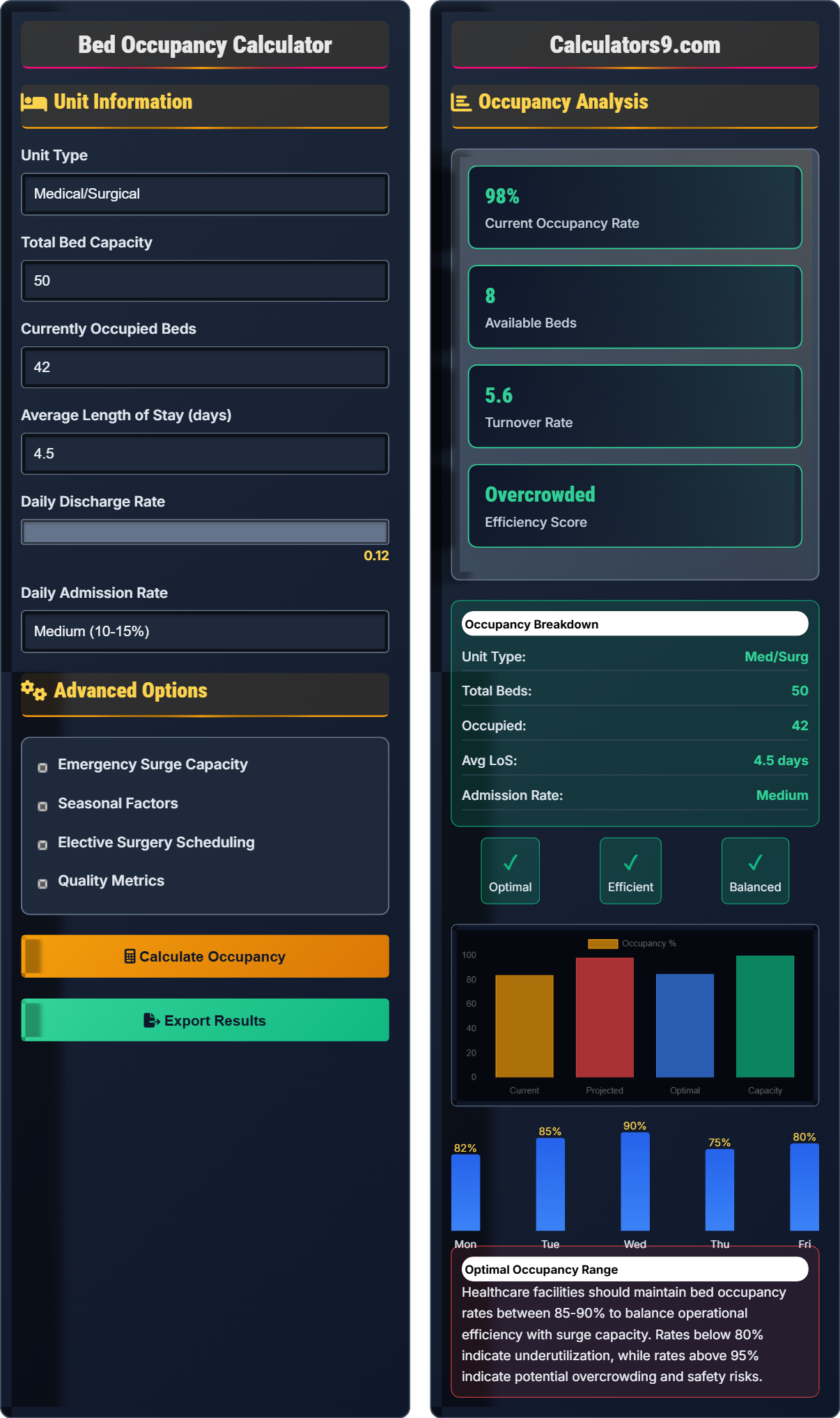
This formula calculates hospital bed occupancy rates based on current utilization and operational factors. Optimal bed occupancy is typically 85-90% to balance efficiency with surge capacity needs.
Example: For a unit with \( OC = 45 \) occupied beds, \( TC = 50 \) total beds, \( DF = 0.1 \) (10% discharge rate), \( EF = 0.05 \) (5% efficiency improvement), and \( AF = 0.08 \) (8% admission rate):
\( BO = \frac{45}{50} \times 100 \times (1 + 0.1) \times (1 - 0.05) \times (1 + 0.08) = 90 \times 1.1 \times 0.95 \times 1.08 = 101.5\% \)
Thus, the projected bed occupancy rate would be 101.5%, indicating overcrowding.
Unit Information
Advanced Options
Occupancy Analysis
Healthcare facilities should maintain bed occupancy rates between 85-90% to balance operational efficiency with surge capacity. Rates below 80% indicate underutilization, while rates above 95% indicate potential overcrowding and safety risks.
Bed Occupancy Framework
Hospital bed occupancy rates are critical metrics for operational efficiency and patient safety. The optimal range is typically 85-90%, balancing efficiency with the need for surge capacity. Rates below 80% indicate underutilization of resources, while rates above 95% suggest potential overcrowding and compromised patient care.
The standard hospital bed occupancy rate calculation uses the following formula:
Where:
- \(BO\) = Bed Occupancy Rate (%)
- \(OC\) = Occupied Beds Count
- \(TC\) = Total Bed Capacity
- \(DF\) = Discharge Factor
- \(EF\) = Efficiency Factor
- \(AF\) = Admission Factor
Healthcare facilities track various metrics related to bed occupancy:
- Bed Turnover Rate: Number of patients per bed per period
- Average Length of Stay: Mean days per patient
- Bed Days Available: Total bed capacity × days in period
- Bed Days Occupied: Actual patient days in period
- Bed Utilization Rate: Percentage of beds in use
- Emergency Admissions: Unscheduled admissions percentage
- Discharge Planning: Proactive planning to reduce LoS
- Capacity Management: Dynamic allocation of resources
- Admission Control: Scheduled admissions to smooth flow
- Efficiency Improvements: Process optimization to reduce delays
- Seasonal Planning: Adjust capacity for seasonal demands
- Surge Protocols: Emergency capacity activation plans
Occupancy Framework
Occupied beds, total capacity, and operational factors determine bed occupancy rates.
\(BO = \frac{OC}{TC} \times 100 \times (1 + DF) \times (1 - EF) \times (1 + AF)\)
Where BO=occupancy rate, OC=occupied beds, TC=total capacity, DF=discharge factor, EF=efficiency factor, AF=admission factor.
- Optimal: 85-90% occupancy
- Underutilized: < 80% occupancy
- Overcrowded: > 95% occupancy
Capacity Analysis
Unit type, patient flow, and operational efficiency influence bed utilization.
- Assess current bed utilization
- Forecast demand patterns
- Plan capacity adjustments
- Monitor performance metrics
- Unit type affects optimal occupancy
- Seasonal variations impact demand
- Surge capacity is essential
Bed Occupancy Learning Quiz
What is the optimal bed occupancy rate for most general medical/surgical units according to healthcare standards?
The answer is B) 85-90%. The optimal bed occupancy rate for general medical/surgical units is 85-90%. This range balances operational efficiency with the need for surge capacity and prevents overcrowding that could compromise patient safety.
Healthcare bed occupancy rates are carefully managed to optimize both efficiency and safety. Rates below 80% indicate underutilization of resources, while rates above 95% suggest overcrowding. The 85-90% range provides a buffer for unexpected admissions while maintaining operational efficiency.
Bed Occupancy Rate: Percentage of beds in use
Surge Capacity: Additional capacity for emergency situationsOperational Efficiency: Effective use of resources
• Optimal range: 85-90%
• Underutilized: < 80%
• Overcrowded: > 95%
• Monitor trends regularly
• Plan for seasonal variations
• Maintain buffer capacity
• Aiming for 100% occupancy
• Not considering surge capacity
• Ignoring seasonal patterns
Calculate the bed occupancy rate for a unit with 45 occupied beds out of 50 total beds, with a discharge factor of 0.1 (10%), efficiency factor of 0.05 (5%), and admission factor of 0.08 (8%). Show your work.
Using the occupancy formula: \(BO = \frac{OC}{TC} \times 100 \times (1 + DF) \times (1 - EF) \times (1 + AF)\)
Given:
- OC = 45 occupied beds
- TC = 50 total beds
- DF = 0.1 (discharge factor)
- EF = 0.05 (efficiency factor)
- AF = 0.08 (admission factor)
Step 1: Calculate base occupancy
Base occupancy = (45/50) × 100 = 90%
Step 2: Apply factors
BO = 90 × (1 + 0.1) × (1 - 0.05) × (1 + 0.08)
= 90 × 1.1 × 0.95 × 1.08
= 90 × 1.1286 = 101.57%
The projected bed occupancy rate is 101.6%, indicating overcrowding.
This calculation demonstrates how operational factors can significantly impact bed occupancy rates. The discharge factor increases the rate (more turnover), the efficiency factor decreases it (better utilization), and the admission factor increases it (more admissions). The final result of 101.6% indicates the unit is overcrowded and needs to take corrective action.
Discharge Factor (DF): Adjusts for patient turnover rate
Efficiency Factor (EF): Reflects operational improvements
Admission Factor (AF): Accounts for new patient inflow
• Base calculation: (occupied/total) × 100
• Add 1 to positive factors
• Subtract from 1 for efficiency factors
• Calculate base rate first
• Apply factors sequentially
• Interpret results against optimal range
• Forgetting to multiply by 100
• Misapplying efficiency factor
• Not interpreting results contextually
An ICU unit has 20 beds with an average length of stay of 5 days. The unit currently has 18 patients (90% occupancy). If the hospital expects a 15% increase in admissions next month and discharge planning efficiency improves by 10%, calculate the new projected occupancy rate. Should the unit consider expanding capacity?
Step 1: Calculate current factors
Current occupancy = 18/20 × 100 = 90%
Step 2: Apply changes
Admission increase factor = 1 + 0.15 = 1.15
Efficiency improvement factor = 1 - 0.10 = 0.90
Step 3: Calculate new occupancy
New occupancy = 90 × 1.15 × 0.90 = 90 × 1.035 = 93.15%
With 93.15% occupancy, the unit is approaching overcrowding (above 95% threshold). The unit should consider expanding capacity or improving discharge processes further.
This example shows how multiple factors interact to affect bed occupancy. ICU units typically have lower optimal occupancy rates (70-85%) due to the critical nature of care and need for immediate availability. A 93% occupancy rate in an ICU indicates significant strain on resources and potential safety risks.
Average Length of Stay (ALOS): Mean days per patient
Capacity Planning: Managing resources to meet demand
Surge Capacity: Extra capacity for emergencies
• ICU optimal: 70-85% occupancy
• General units: 85-90% occupancy
• >95% indicates overcrowding
• Consider unit-specific optimal ranges
• Plan ahead for capacity needs
• Monitor trends over time
• Using same targets for all unit types
• Not accounting for unit-specific needs
• Ignoring trend analysis
A pediatric unit has 30 beds with current occupancy of 24 beds (80%). During flu season, admissions typically increase by 40%, but the average length of stay decreases by 20% due to proactive care protocols. Calculate the projected occupancy during flu season and determine if the unit needs temporary capacity expansion.
Step 1: Calculate current occupancy
Current occupancy = 24/30 × 100 = 80%
Step 2: Calculate seasonal factors
Admission increase = 1 + 0.40 = 1.40
LOS decrease factor = 1 - 0.20 = 0.80 (faster turnover)
Step 3: Calculate new occupancy
Projected occupancy = 80 × 1.40 × 0.80 = 80 × 1.12 = 89.6%
The projected occupancy of 89.6% is within the optimal range (85-90%) for a pediatric unit, so temporary expansion is not needed.
This demonstrates how seasonal factors can have opposing effects on occupancy. Increased admissions tend to increase occupancy, but decreased length of stay (due to efficiency improvements) tends to decrease occupancy by increasing turnover. The net effect depends on the relative magnitude of these factors.
Seasonal Variation: Changes in demand based on time of year
Length of Stay Reduction: Improving patient throughput
Capacity Expansion: Adding temporary or permanent beds
• Seasonal planning requires historical data
• Opposing factors can offset each other
• Consider optimal range for unit type
• Analyze historical seasonal patterns
• Consider both demand and efficiency factors
• Plan capacity adjustments in advance
• Only considering demand factors
• Ignoring efficiency improvements
• Not accounting for unit-specific ranges
How does bed overcrowding (occupancy rates > 95%) typically impact healthcare quality metrics?
The answer is C) Increases infection rates, readmissions, and staff burnout. Bed overcrowding leads to increased infection transmission, longer wait times for care, staff fatigue, and reduced quality of care. Studies show that occupancy rates above 95% correlate with worse patient outcomes and higher staff turnover.
Research has consistently shown that hospitals with occupancy rates above 95% experience decreased quality metrics. The Institute for Healthcare Improvement and other organizations recommend maintaining occupancy below 95% to preserve quality care. High occupancy reduces staff ability to provide individualized attention and increases stress on the system.
Quality Metrics: Measures of healthcare performance
Readmission Rates: Patients returning within 30 days
Staff Burnout: Physical and emotional exhaustion
• >95% occupancy degrades quality
• Optimal range balances efficiency and safety
• Quality metrics decline with overcrowding
• Monitor quality metrics with occupancy
• Set maximum thresholds
• Plan for surge capacity
• Prioritizing 100% occupancy over quality
• Not tracking quality metrics
• Ignoring staff feedback on capacity
Healthcare Operations FAQ
Q: How does average length of stay (ALOS) affect bed occupancy rates?
A: Average Length of Stay (ALOS) has an inverse relationship with bed turnover and occupancy rates. A shorter ALOS increases bed turnover, which can decrease occupancy rates if demand remains constant. Conversely, a longer ALOS reduces turnover, potentially increasing occupancy.
Using our formula: \( BO = \frac{OC}{TC} \times 100 \times (1 + DF) \times (1 - EF) \times (1 + AF) \), ALOS primarily affects the Discharge Factor (DF).
For example, if a unit has 40 occupied beds out of 50 total beds (80% base occupancy):
With high ALOS (DF = 0.05): \( BO = 80 \times (1 + 0.05) = 84\% \)
With low ALOS (DF = 0.20): \( BO = 80 \times (1 + 0.20) = 96\% \)
However, lower ALOS usually indicates better care efficiency, which is generally positive despite the higher occupancy rate.
Q: What's the relationship between bed occupancy and patient safety?
A: There's a critical relationship between bed occupancy and patient safety, with an optimal range around 85-90%. Research shows that occupancy rates above 95% correlate with:
• Increased infection rates (OR 1.15-1.30 for HAIs)
• Higher readmission rates (increased by 5-10%)
• Longer wait times for care
• Increased staff burnout and turnover
• Reduced individualized patient attention
For a unit with 50 beds operating at 98% occupancy (49 beds filled):
Each nurse might manage 6-7 patients instead of the optimal 4-5, reducing time for individual assessments and interventions. This strain on the system can compromise safety protocols and increase adverse events.
The goal is to balance efficiency with the safety buffer that comes from having available beds for emergencies and individualized care.