Staffing Ratio Calculator
Healthcare operations tool • 2026 edition
Staffing Ratio Formula:
Show the calculator\( SR = \frac{P}{S \times H \times (1 - U) \times (1 + C) \times (1 - E)} \)
Where:
- \( SR \) = Staffing Ratio (patients per staff member)
- \( P \) = Patient Volume (number of patients)
- \( S \) = Staff Count (number of staff members)
- \( H \) = Hours of Operation (shift length)
- \( U \) = Utilization Factor (absences, breaks)
- \( C \) = Complexity Factor (patient acuity)
- \( E \) = Efficiency Factor (process improvements)
This formula calculates healthcare staffing ratios based on patient volume, staff availability, and operational factors. Regulatory standards vary by department and patient acuity level, with ICU typically requiring 1:2 ratios and general wards 1:4-1:6.
Example: For a unit with \( P = 30 \) patients, \( S = 8 \) nurses, \( H = 12 \)-hour shifts, \( U = 0.15 \) (15% unavailable time), \( C = 0.25 \) (25% complexity adjustment), and \( E = 0.1 \) (10% efficiency improvement):
\( SR = \frac{30}{8 \times 12 \times (1 - 0.15) \times (1 + 0.25) \times (1 - 0.1)} = \frac{30}{8 \times 12 \times 0.85 \times 1.25 \times 0.9} = \frac{30}{73.8} \approx 0.41 \)
This translates to approximately 1:2.4 staffing ratio (about 2.4 patients per nurse).
Unit Information
Advanced Options
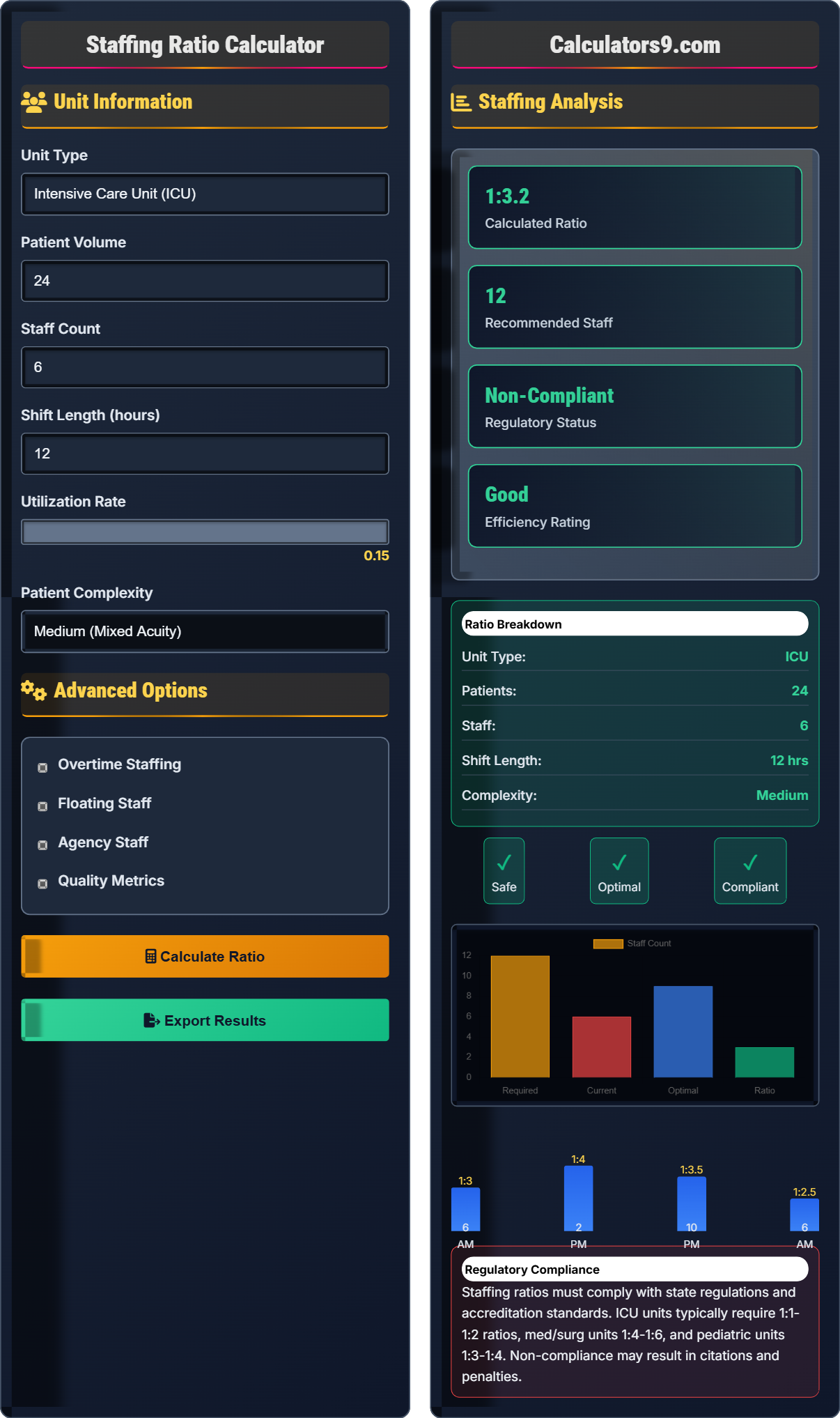
Staffing Analysis
Staffing ratios must comply with state regulations and accreditation standards. ICU units typically require 1:1-1:2 ratios, med/surg units 1:4-1:6, and pediatric units 1:3-1:4. Non-compliance may result in citations and penalties.
Staffing Ratio Framework
Healthcare staffing ratios are regulated by state nursing boards and accreditation agencies. These ratios ensure safe patient care and optimal outcomes. Staffing requirements vary by unit type, patient acuity, and regulatory jurisdiction. Maintaining appropriate ratios is critical for quality care and regulatory compliance.
The standard healthcare staffing ratio calculation uses the following formula:
Where:
- \(SR\) = Staffing Ratio (patients per staff member)
- \(P\) = Patient Volume
- \(S\) = Staff Count
- \(H\) = Hours of Operation
- \(U\) = Utilization Factor
- \(C\) = Complexity Factor
- \(E\) = Efficiency Factor
Healthcare facilities must comply with various staffing standards:
- State Regulations: Vary by jurisdiction (e.g., California mandates ICU ratios)
- JCAHO Standards: Joint Commission accreditation requirements
- OIG Guidelines: Federal oversight for Medicare/Medicaid
- Professional Standards: ANA recommendations for safe staffing
- Union Agreements: Collective bargaining agreements
- Quality Metrics: Patient safety indicators and outcomes
- Flexible Scheduling: Adjust staffing based on patient census patterns
- Acuity-Based Staffing: Match staff skill level to patient needs
- Team Nursing: Collaborative care models to maximize efficiency
- Technology Integration: Automated systems to support nursing workflows
- Cross-Training: Develop versatile staff for flexible deployment
- Data Analytics: Predictive modeling for staffing needs
Staffing Framework
Patients, staff, and operational factors determine healthcare staffing ratios.
\(SR = \frac{P}{S \times H \times (1 - U) \times (1 + C) \times (1 - E)}\)
Where SR=staffing ratio, P=patients, S=staff, H=hours, U=utilization, C=complexity, E=efficiency.
- ICU: 1:1-1:2 ratio
- Med/Surg: 1:4-1:6 ratio
- Pediatrics: 1:3-1:4 ratio
Ratio Analysis
Unit type, patient acuity, and operational efficiency influence staffing ratios.
- Assess patient volume and acuity
- Determine required staff count
- Apply operational factors
- Verify regulatory compliance
- Unit type affects required ratios
- Higher acuity requires more staff
- Efficiency can optimize ratios
Staffing Ratio Learning Quiz
What is the recommended staffing ratio for a general medical/surgical unit according to most regulatory standards?
The answer is C) 1:4-1:6 (nurse to patients). Most regulatory standards recommend 1:4 to 1:6 nurse-to-patient ratios for general medical/surgical units. This ratio balances patient safety with operational efficiency.
Healthcare staffing ratios are evidence-based standards developed to ensure patient safety and quality care. The 1:4-1:6 ratio for med/surg units reflects the balance between providing adequate care and managing operational costs. These ratios are enforced by regulatory bodies like JCAHO and state nursing boards.
Staffing Ratio: Proportion of staff to patients
Regulatory Standards: Requirements set by governing bodies
Medical/Surgical Unit: General care ward for stable patients
• ICU: 1:1-1:2 recommended
• Med/Surg: 1:4-1:6 recommended
• Pediatric: 1:3-1:4 recommended
• Know unit-specific ratios
• Monitor compliance regularly
• Adjust for patient acuity
• Confusing ratios for different unit types
• Not considering patient acuity
• Ignoring regulatory requirements
Calculate the staffing ratio for a unit with 30 patients, 8 nurses working 12-hour shifts, with 15% utilization factor (breaks, absences), 25% complexity factor for patient acuity, and 10% efficiency factor from process improvements. Show your work.
Using the staffing ratio formula: \(SR = \frac{P}{S \times H \times (1 - U) \times (1 + C) \times (1 - E)}\)
Given:
- P = 30 patients
- S = 8 nurses
- H = 12 hours
- U = 0.15 (utilization factor)
- C = 0.25 (complexity factor)
- E = 0.10 (efficiency factor)
Step 1: Calculate denominator components
Effective staff time = S × H × (1 - U) = 8 × 12 × (1 - 0.15) = 8 × 12 × 0.85 = 81.6
Step 2: Apply complexity and efficiency factors
Adjusted capacity = 81.6 × (1 + 0.25) × (1 - 0.10) = 81.6 × 1.25 × 0.9 = 91.8
Step 3: Calculate ratio
SR = 30 / 91.8 = 0.327
This means approximately 1:3.06 ratio, or about 3 patients per nurse.
This calculation demonstrates how multiple factors affect staffing capacity. The utilization factor reduces effective staff time, while complexity increases demand. Efficiency improvements partially offset these effects. The final ratio shows that despite having 8 nurses for 30 patients (1:3.75), the adjusted ratio is 1:3.06 due to various operational factors.
Utilization Factor (U): Accounts for non-productive time
Complexity Factor (C): Adjusts for patient acuity
Efficiency Factor (E): Reflects process improvements
• Subtract utilization from 1
• Add complexity to 1
• Subtract efficiency from 1
• Calculate denominator first
• Apply factors sequentially
• Convert to patient-per-staff format
• Misapplying the mathematical operations
• Forgetting to convert to standard ratio format
• Incorrectly handling factor signs
An ICU unit has 12 critical care patients requiring 1:1 or 1:2 staffing ratios depending on acuity. If 60% of patients require 1:1 care and the rest require 1:2 care, how many nurses are needed to meet regulatory requirements? If the unit currently has 10 nurses, is it compliant?
Step 1: Calculate patient distribution
1:1 care patients = 12 × 0.6 = 7.2 ≈ 7 patients
1:2 care patients = 12 × 0.4 = 4.8 ≈ 5 patients
Step 2: Calculate required staff
For 1:1 patients: 7 × 1 = 7 nurses
For 1:2 patients: 5 ÷ 2 = 2.5 ≈ 3 nurses
Total required nurses = 7 + 3 = 10 nurses
Step 3: Assess compliance
The unit currently has 10 nurses, which meets the minimum requirement. It is compliant but has no buffer for breaks, lunches, or emergencies.
This example shows how mixed acuity levels affect staffing requirements. ICU units often have a combination of patients requiring different levels of care. The calculation demonstrates that you can't simply average the ratios; each patient category must be calculated separately and then summed.
Acuity: Severity level of patient condition
Regulatory Compliance: Meeting required standards
Critical Care: Intensive monitoring and intervention
• Calculate each acuity level separately
• Sum required staff for all categories
• Include buffer for operational needs
• Group patients by acuity level
• Calculate staff requirements separately
• Add buffer for operational needs
• Averaging ratios instead of calculating separately
• Forgetting to account for breaks/lunches
• Not considering regulatory buffer requirements
A medical/surgical unit has 30 patients with an average of 1:5 nurse-to-patient ratio. The unit operates 24/7 with 12-hour shifts and wants to achieve 1:4 ratios during day shift (7 AM-7 PM) and maintain 1:5 during night shift (7 PM-7 AM). Calculate the required staffing for each shift and the total daily staffing cost if day shift nurses earn $60/hour and night shift nurses earn $65/hour.
Step 1: Calculate required staff for each shift
Day shift (1:4 ratio): 30 ÷ 4 = 7.5 ≈ 8 nurses
Night shift (1:5 ratio): 30 ÷ 5 = 6 nurses
Step 2: Calculate daily staffing cost
Day shift cost: 8 nurses × 12 hours × $60/hour = $5,760
Night shift cost: 6 nurses × 12 hours × $65/hour = $4,680
Total daily cost: $5,760 + $4,680 = $10,440
The unit needs 14 total nurses per day (8 day shift, 6 night shift) at a cost of $10,440.
This demonstrates how operational requirements affect staffing costs. By optimizing ratios during busier day shifts, the unit improves patient care while managing costs. The differential pay rate reflects premium compensation for night shift work, which is standard practice in healthcare.
Shift Differential: Premium pay for less desirable shifts
Optimization: Balancing care quality with costs
24/7 Operations: Continuous care requiring shift coverage
• Calculate ratios separately by shift
• Account for shift differential in costs
• Ensure 24-hour coverage
• Plan staffing by shift requirements
• Consider patient census patterns
• Factor in shift differential costs
• Not accounting for shift differential
• Calculating average ratios instead of shift-specific
• Forgetting to ensure 24-hour coverage
How does inadequate staffing (higher patient-to-nurse ratios) typically impact healthcare quality metrics?
The answer is C) Increases patient falls, infections, and mortality. Research consistently shows that higher patient-to-nurse ratios correlate with adverse outcomes including increased patient falls, hospital-acquired infections, medication errors, and mortality rates. Adequate staffing is essential for quality patient care.
Extensive research, including studies by Aiken et al., has demonstrated the direct correlation between nurse staffing ratios and patient outcomes. The landmark study showed that each additional patient per nurse increased the risk of death by 7%. This evidence forms the basis for regulatory staffing standards.
Quality Metrics: Measures of healthcare performance
Adverse Outcomes: Negative patient events
Research Evidence: Studies supporting staffing standards
• Higher ratios = worse outcomes
• Adequate staffing improves safety
• Regulatory standards are evidence-based
• Use evidence to justify staffing
• Monitor quality metrics
• Link staffing to outcomes
• Assuming cost savings justify poor ratios
• Not tracking outcome correlations
• Ignoring research evidence
Healthcare Operations FAQ
Q: How does patient acuity affect staffing requirements in healthcare facilities?
A: Patient acuity significantly impacts staffing through the complexity factor \( C \) in our staffing formula: \( SR = \frac{P}{S \times H \times (1 - U) \times (1 + C) \times (1 - E)} \).
For example, if we have 24 patients in a med/surg unit:
With low acuity (C = 0.1): \( SR = \frac{24}{6 \times 12 \times (1 - 0.15) \times (1 + 0.1) \times (1 - 0.05)} = \frac{24}{6 \times 12 \times 0.85 \times 1.1 \times 0.95} = \frac{24}{50.8} \approx 1:2.1 \)
With high acuity (C = 0.5): \( SR = \frac{24}{6 \times 12 \times (1 - 0.15) \times (1 + 0.5) \times (1 - 0.05)} = \frac{24}{6 \times 12 \times 0.85 \times 1.5 \times 0.95} = \frac{24}{86.7} \approx 1:3.6 \)
Higher acuity increases staffing needs by requiring more nursing time per patient, effectively reducing the number of patients each nurse can safely manage.
Q: What's the relationship between staffing ratios and healthcare costs?
A: The relationship between staffing ratios and costs is complex, involving both direct and indirect costs. While improved staffing ratios increase direct labor costs, they often reduce total costs through better outcomes.
Direct costs for a unit with 30 patients:
At 1:5 ratio: 6 nurses × $60/hr × 24 hrs = $8,640/day
At 1:4 ratio: 8 nurses × $60/hr × 24 hrs = $11,520/day
Indirect savings (per Aiken study): 1:4 ratio reduces complications by 15-20%, saving $1,500-3,000 per patient in reduced length of stay and fewer readmissions.
For 30 patients: Potential savings of $45,000-90,000 per month in reduced complications, often offsetting increased staffing costs.
The optimal staffing balance considers both immediate labor costs and long-term quality outcomes.